Creatine, once the preserve of the gym obsessed and source of memes around the excessively jacked, has transcended its initial reputation as a muscle-builder to become a subject of intense scientific scrutiny for a wide array of health and performance applications - and hence in the news almost daily at the moment.

But what actually is it? What’s its physiological role, what can it do for physical and cognitive performance, and could it potentially stave off aging or cure critical illness? And how certain are we?
Before you read any further: This is not medical advice - just a summary of the evidence around creatine and it’s many and varied uses. Although we will discuss the safety profile of creatine, you should always seek your own personalised advice from a health professional if you’re tempted to use it yourself.
Creatine is a naturally occurring nitrogenous organic acid, synthesised in the liver, kidneys, and pancreas from the amino acids arginine, glycine, and methionine. It’s also obtained directly from red meat and seafood, which is the source of about 50% of the 1-3g you ordinarily use per day.
Approximately 95% of the body’s creatine is stored in skeletal muscle, with the remainder in the brain and other tissues. Within cells, about two-thirds of creatine exists as phosphocreatine (PCr), and it’s here that its primary physiological function lies. within the ATP-PCr energy system:
- Adenosine Triphosphate (ATP) is the cell’s immediate energy currency.
- During high-intensity, short-duration activities like sprinting of lifting heavy weights, ATP is rapidly depleted.
- PCr serves as a readily available phosphate reserve, quickly donating its phosphate group to adenosine diphosphate (ADP) to regenerate ATP, a reaction catalyzed by creatine kinase.
- This system sustains maximal power output for roughly 5-10 seconds, before other energy systems (eg glycolysis) take over.
- Creatine supplementation increases intramuscular PCr stores, enhancing this rapid ATP regeneration capacity.
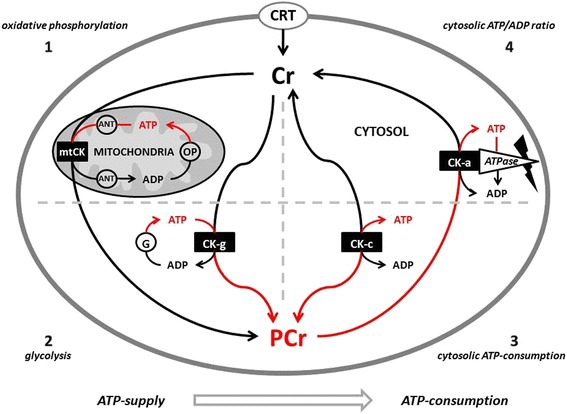
Beyond direct energy buffering, creatine is also involved in the “creatine phosphate shuttle” between mitochondria and sites of energy use, helping to maintain ATP/ADP ratios in active tissue, buffering changes in pH, and may have indirect antioxidant effects through reducing the formation of reactive oxygen species. There’s also evidence that it may also reduce protein breakdown, stabilise cell membranes, enhance glycogen storage when consumed with carbohydrates, and influence pathways involved in muscle growth.
So it’s not merely about providing more instantly available muscle fuel - creatine seems to be involved in fostering an overall more resilient and adaptive cellular environment, which likely explains the ongoing discovery of new potential applications for creatine.
The effect of creatine on physical performance
Creatine’s impact on athletic performance is its most well-known application, but its effects vary depending on the type of activity.

Creatine monohydrate is widely recognised as one of the most effective legal ergogenic aids for enhancing high-intensity exercise capacity and lean body mass. By boosting PCr stores, it allows for more work to be performed during resistance training, leading to greater gains in strength and muscle hypertrophy over time. Numerous meta-analyses confirm that creatine supplementation combined with resistance training significantly improves muscle strength and lean body mass in both younger and older adults.
Some evidence suggests potential sex-based differences in response, with a few meta-analyses indicating potentially larger strength and LBM gains in males compared to females. However, significant benefits are still clearly documented in females, especially older women, and more research focusing specifically on female physiology and response is needed, as past studies may have had methodological limitations that resulted in bias.
One criticism of creatine is that the initial rapid weight (and aesthetic!) gain seems to be due to water retention in muscle cells, however longer-term gains have been clearly demonstrated to reflect genuine increase in muscle protein content and tissue accrual.
The effect of creatine on endurance performance is less straightforward. It generally does not enhance performance in prolonged, steady-state aerobic activities, and some research even suggests a potential slight negative impact on VO2max. However, creatine can be beneficial in endurance sports that feature intermittent high-intensity efforts, such as sprints, climbs, or surges. This is attributed to its ability to enhance anaerobic work capacity, improve acid buffering, and potentially aid glycogen resynthesis when co-ingested with carbohydrates.
Supporting this nuanced view, studies have demonstrated benefits for repeated sprint performance, increased interval power output during endurance cycling tests, improved performance on anaerobic tests in football players, and an increased time to exhaustion during high-intensity endurance tasks.
The conflicting data on creatine and endurance likely arises from differences in how “endurance” is defined and measured. As we’ve discussed, creatine primarily boosts the ATP-PCr system, crucial for anaerobic efforts. Purely aerobic activities relying exclusively on oxidative phosphorylation, like steady-state running or a flat cycling time trial, may see little benefit - or even a slight hindrance from the associated weight gain. However, many real-world endurance sports including cycling (anyone who has seen me race on Zwift will notice my efforts are anything but steady-state), triathlon, middle-distance running, and team-sports like football or rugby have crucial moments like climbs, breakaways, surges, or finishing sprints where anaerobic capacity is important. In these contexts, creatine’s ability to enhance high-intensity work capacity within the endurance event can be advantageous.
Beyond brawn: Creatine and the brain
The brain is hungry, consuming a disproportionate amount of the body’s total energy budget despite its relatively small size. Maintaining a constant supply of ATP is therefore crucial, so similar to muscle cells, neurons use PCr as an energy buffer to rapidly regenerate ATP during periods of high metabolic demand.
Research into whether creatine supplementation enhances cognitive function in healthy individuals has yielded mixed results. It’s clear that supplementation can increase creatine levels within the brain, although this process appears slower and potentially requires higher doses or longer durations compared to muscle saturation. But what does this mean for neuropsychiatric outcomes?
Some meta-analyses suggest benefits, particularly for memory, with more pronounced effects in older adults. Cognitive benefits might also be more apparent under conditions of metabolic stress, like sleep deprivation or hypoxia. Supplementation potentially improved attention time and information processing speed, but no significant overall improvement in general cognitive function or executive functions (like planning, inhibition, and working memory).
Reflecting this uncertainty, the European Food Safety Authority (EFSA) panel reviewed the evidence in 2024 and concluded that a causal relationship between creatine supplementation and improved cognitive function has not been established, citing inconsistent findings across studies, a lack of clear dose-response relationships, isolated positive results among many tests performed, and relatively weak evidence for the proposed mechanisms in healthy individuals.
Outside of this, the potential for creatine in treating conditions like traumatic brain injury or psychiatric disorders is an active area of research but requires more evidence.
The impact on general health and aging
Creatine’s potential applications extend beyond athletic performance and cognition, touching upon aspects of aging and broader clinical health.
Sarcopenia, the age-related decline in muscle mass, strength, and function, is a major contributor to frailty, reduced mobility, and decreased quality of life in older adults. Resistance training (RT) is a cornerstone intervention to combat sarcopenia, and multiple meta-analyses shows that adding creatine supplementation to RT significantly enhances gains in lean tissue mass and muscle strength in adults aged 55 and older. This combination may also lead to better functional performance, such as improved ability to rise from a chair, and potentially reduce the risk of falls.
The effects of creatine on bone health are more nuanced. Osteoporosis, characterised by low bone mineral density (BMD) and increased fracture risk, is another significant concern with aging, particularly for postmenopausal women. Theoretically, creatine could benefit bone through several mechanisms: directly stimulating bone-forming osteoblasts, reducing the activity of bone-resorbing osteoclasts, and indirectly by increasing muscle mass and strength, applying greater mechanical and hence stimulating bone maintenance and growth. However, meta-analyses generally found no significant additive benefit of creatine supplementation (combined with exercise) on BMD compared to exercise alone, and a 2-year RCT involving over 200 postmenopausal women undergoing resistance training and walking found no difference in BMD changes between the creatine and placebo groups, although it did find a subtle positive effect on bone structure which might influence fracture resistance, even without increasing overall density.
What about creatine in critical illness?
As an intensivist, I tend to view most therapies through the lens of “can this help the sickest people in the hospital?”. Critically ill patients in ICU often experience rapid and severe muscle wasting linked to multiple factors like disuse, inflammation, and impaired cellular energy metabolism, including depleted muscle PCr and creatine levels. This muscle loss can be rapid - around 15% over the first week on ICU - and is associated with prolonged ventilation, poor recovery, and increased mortality.
Currently, there are no proven, consistently effective interventions specifically targeting muscle preservation in the critically unwell, however low serum creatinine levels upon admission, often used as a rough indicator of muscle mass, have been shown to predict higher mortality rates, highlighting the link between muscle status and survival in critical illness.
Theoretically, creatine supplementation could help by replenishing muscle energy stores and supporting muscle protein synthesis. By potentially boosting the muscle’s energy reserves, creatine might help counteract the bioenergetic failure associated with muscle wasting, support protein synthesis (especially when combined with adequate protein and calorie intake, alongside early and agressive exercise and mobilisation), and perhaps attenuate muscle breakdown? The profound disruption of muscle energy metabolism seen in critical illness suggests that simply providing nutritional building blocks like protein may be insufficient if the muscle cells lack the necessary energy to utilise them effectively for repair and maintenance, so augmenting the ATP-PCr system may have a role here.
Current evidence supporting creatine use in critical illness is limited, but suggestive of potential. Systematic reviews examining nutritional strategies to combat muscle wasting in critical illness have identified creatine, along with other agents like leucine and β-hydroxy-β-methylbutyrate, as interventions that warrant further investigation.
However, we don’t yet have large-scale clinical trials that have specifically tested the efficacy and safety of creatine supplementation in this vulnerable population, but as a relatively inexpensive and generally safe compound (in other populations), creatine potentially represents a promising candidate to determine if it can help mitigate muscle wasting and improve patient outcomes. A study in acute stroke patients (a condition with some metabolic similarities to critical illness) did not find benefits for muscle mass or function with creatine, though it did note a reduction in markers of inflammation, which may be of benefit given the link between chronic inflammation and the post-intensive care syndrome.
Are we sure that it is safe?
Creatine monohydrate is one of the most extensively studied nutritional supplements available, with decades of use - and research - underpinning its safety at a population level.
Numerous position statements from the International Society of Sports Nutrition and others consistently affirm that creatine supplementation is safe for healthy individuals across various age groups, for both short-term and long-term use. Studies involving supplementation durations of up to 5 years, with doses as high as 30 g/day, failed to reveal significant adverse health effects, and analysis of millions of adverse event reports submitted to regulatory agencies globally shows that creatine is mentioned extremely rarely, supporting the trials findings.
The persistent claim that creatine harms kidneys is largely unfounded in healthy individuals. Creatine supplementation increases serum creatinine (a breakdown product), which is a marker used to estimate kidney function. However this rise reflects increased creatine turnover, not kidney damage, and studies using direct measures of kidney function and other biomarkers confirm its safety for healthy kidneys. However, caution is advised for those with pre-existing kidney disease, or taking nephrotoxic drugs.
Another common misconception is that creatine causes dehydration and muscle cramps, arising from the fact that creatine draws water into muscle cells as it accumulates there. However research suggests the opposite may be true, and creatine supplementation might reduce the risk of cramping and heat-related illness during exercise, especially in hot environments. The ISSN review discusses studies involving athletes undergoing intense training have found no increase, and sometimes even a decrease, in the incidence of dehydration or muscle cramps among those using creatine compared to controls.
As mentioned earlier, creatine supplementation typically causes a rapid increase in body weight, which may be around 1-2 kg during the first week if a “loading” dose is used. However, this is primarily due to water retention within the muscle cells, driven by the osmotic effect of increased intracellular creatine concentration.
The most commonly reported side effect, though still relatively infrequent, is GI discomfort including nausea and diarrhea. These effects are more likely to occur with higher doses, particularly if large single doses (e.g., 10 grams or more) are taken at once, or if creatine is consumed without sufficient fluids, and occur only slightly more prevalently with creatine than with placebo.
Finally, a single study showed increased dihydrotestosterone with creatine, a hormone linked to hair loss, but did not report actual hair loss. Subsequent reviews found no consistent effect on DHT or direct link to hair loss, and anecdotal reports linking creatine to acne, compartment syndrome, or rhabdomyolysis are not substantiated by scientific evidence.
Concerns about unknown long-term effects are largely mitigated by how many athletes have been using creatine and for how long. Studies tracking individuals using creatine for extended periods have consistently reported a lack of significant adverse health effects. Long term serial blood tests assessing markers of metabolic, liver, muscle, and kidney health have shown no negative impact from long-term supplementation in athletes compared to non-users.
But what does all this practically mean?
Based on the evidence, creatine supplementation is most likely to be beneficial for:
- People engaging in resistance training, seeking improvements in muscle strength, power output, and lean body mass.
- Athletes in sports requiring repeated high-intensity bursts, such as team sports, track athletes, cyclists, and weightlifters.
- Older adults aiming to counteract age-related muscle loss and maintain physical function
- Vegetarians and vegans, as as their baseline muscle creatine stores are typically lower.
- People seeking potential cognitive support, especially if under conditions of significant metabolic stress (eg sleep deprivation), although more research is needed to confirm the consistency and magnitude of these effects.
In terms of dosing, two primary supplementation strategies are used to increase muscle creatine stores, with little evidence of superiority for one over the other.
Most commonly you’ll see a loading and maintainance approach suggested to quickly saturate muscle stores:
- Loading Phase: This typically involves consuming approximately 0.3 grams of creatine monohydrate per kilogram of body weight per day (typically around 20-25 grams daily for most) for 5 to 7 days. It’s recommended that this should be divided into 4-5 smaller doses (e.g., 5 grams taken four times a day) to improve tolerance and absorption.
- Maintenance Phase: After the loading phase (or if skipping the loading phase), a daily dose of 3-5 grams is sufficient to maintain saturated muscle creatine levels. Some research suggests larger individuals or those with very high muscle mass might benefit from slightly higher maintenance doses, potentially in the range of 5-10 grams per day, with potentially higher doses leading to more enhanced cognitive effects.
However, one could skip the loading phase and simply start with the maintenance dose of 3-5 grams per day. This method will saturate muscle stores, but will take longer and the initial performance benefits may also appear more gradually with this approach. Outcomes are typically identical by thirty days.
In terms of timing, some studies suggest that taking creatine post-exercise, possibly combined with carbohydrates and/or protein, might slightly enhance muscle uptake, however the impact of timing on actual performance outcomes compared to taking creatine alone at other times is less clear. The most critical factor for effectiveness is consistent daily intake to keep muscle stores elevated.
Creatine monohydrate is the form used in the vast majority of scientific studies and is consistently shown to be effective and safe. It is also typically the most affordable option. There are various other forms of creatine (including but not limited to creatine ethyl ester, buffered creatine, liquid creatine, creatine hydrochloride, creatine gummies, etc) which are marketed with claims of superior absorption, stability, or reduced side effects. However, there is currently little to no credible scientific evidence to support these claims over creatine monohydrate, potentially lack the safety profile of the monohydrate form through lack of experience of their use, and many are also significantly more expensive.
And after all this, remember that all of this is population level data - individual users will each respond differently to creatine. “Responders” typically see muscle creatine content rise by >20 mmol/kg dry weight, while “non-responders” see increases <10 mmol/kg. Factors like lower baseline muscle creatine levels and a higher percentage of type II muscle fibers may characterise responders.
The tl;dr conclusion
Despite all the recent hype, creatine has been used for decades, making creatine monohydrate one of the most researched nutritional supplements, with a robust body of evidence supporting both its efficacy and safety.
Its ability to enhance muscle strength, power output, and lean mass gains, particularly when combined with resistance training, is well-established across various populations, and while it doesn’t appear to benefit steady-state aerobic capacity it can enhance performance in activities involving intermittent high-intensity efforts by boosting anaerobic capacity, while also offering potential benefits for memory, especially under stressful conditions such as sleep deprivation. Crucially, decades of research overwhelmingly support the safety profile of creatine monohydrate for healthy individuals.
Ultimately however, decisions about creatine supplementation should be individualised and guided by an understanding of the scientific evidence relevant to your own specific goals and health, rather than by anecdotal claims or marketing and media hype.
While creatine monohydrate is typically safe for most healthy individuals, it is always advisable to consult with a healthcare professional (such as your GP, a sports and exercise doctor, or registered dietitian) before starting any new supplement regimen. This is particularly important for individuals with pre-existing medical conditions (especially kidney disease), those taking medications, pregnant or breastfeeding women, and children or adolescents.